Pathophysiology:
Hyponatremia is a disorder of water imbalance
Hyponatremia means excess of body water compared to total body sodium and potassium. Also likely to involve ADH (vasopressin), the hormone involved in water balance.
Total osmolality: concentration of all solutes in a given weight of water (mOsm/kg) regardless of whether or not osmoles move across biological membranes
Effective osmolality: number of osmoles that contribute to water movement between intracellular and extracellular compartments
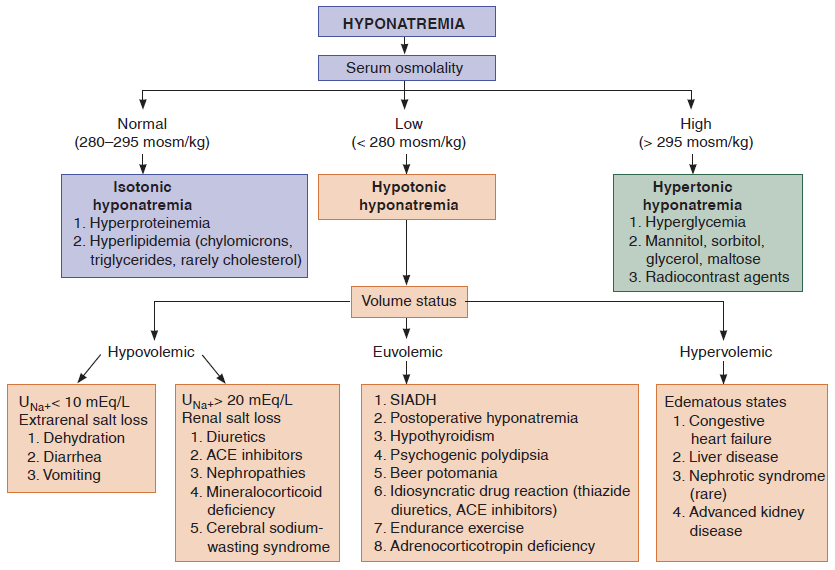
Most hyponatremia is from low effective osmolality (hypo-osmotic/hypotonic hyponatremia), but occasionally, hyponatremia occurs in isotonic or hypertonic serum because other active osmoles are present.
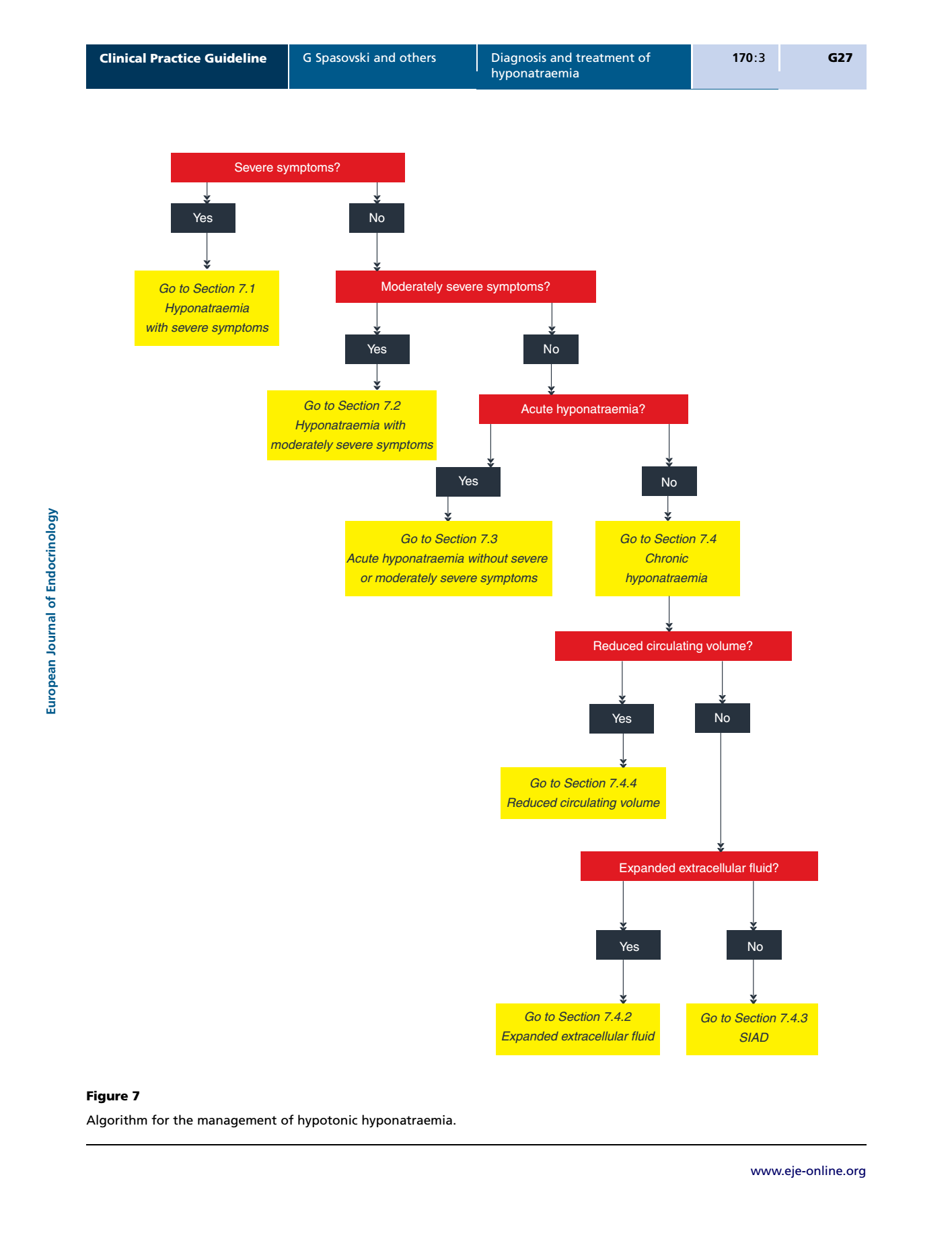
ACUTE vs CHRONIC:
Is there a documented change in sodium within 48 hours?
Basis: when there is rapid hyponatremia (often from excess water), brain takes about 24-28 hours to reduce number of osmotically active particles within its cells to restore brain volume to normal (ie, avoid swelling)
Role of vasopressin (anti-diuretic hormone):
osmo-receptors in hypothalamus sense effective osmolality; baroreceptors in carotid sinus, left atrium, aortic arch will sense what the effective volume is, based on the input from the above receptors, body increase/inhibit ADH secretion accordingly.
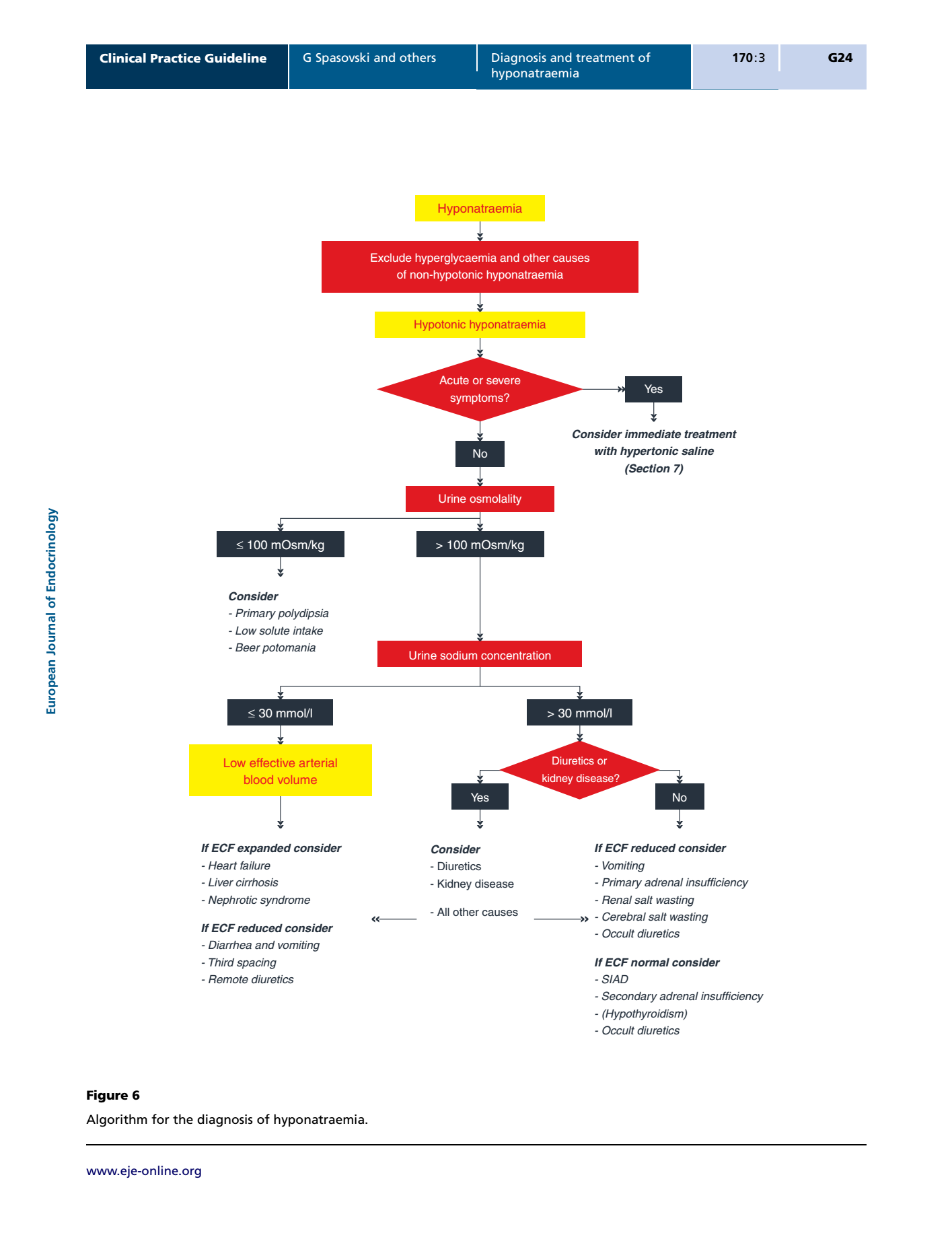
How to evaluate hyponatremia
- Assess Volume status: Is the patient volume overloaded, depleted, or euvolemic?
- Assess Osmolality (hyper, iso, hypo): Is the blood concentrated?
For hypotonic hyponatremia, continue to 3 rd step - Assess Urinary sodium excretion and FeNa %: Is the urine concentrated?
*Remember VOU – volume status, osmolality, and urine studies
Will Fluid restriction work ?
If you decide that patient is Euvolemic or hypervolemic, and would like to try fluid restriction, use Urine ( Na + K ) to evaluate the probability of responsiveness to fluid restriction.
If Serum Na > Urine (Na + K), it means patient's kidney is still able to clear FREE water. And thus patient's hyponatremia will response to fluid restriction
If Serum Na < Urine (Na + K), it means patient's kidney cannot clear FREE water and patient need more solute. Patient need increase salt intake (IV v.s. PO)
Hyponatremia v.s. solute intake
Minimal urine osmolarity ~ 50 mOsm/kg of water
If a person take 650 mOsm daily, one can drink up-to 650/50 (minimal urine osmolarity, i.e. maximal free water excretion) = 13 L of water without causing hyponatremia.
If a person has potomania (beer drinker's hyponatremia), only intake about 200 mOsm daily. Any water intake > 200/50 = 4L will cause hyponatremia.
Edited by Dr. Tan Nguyen, The God of Jacobi RISC