-
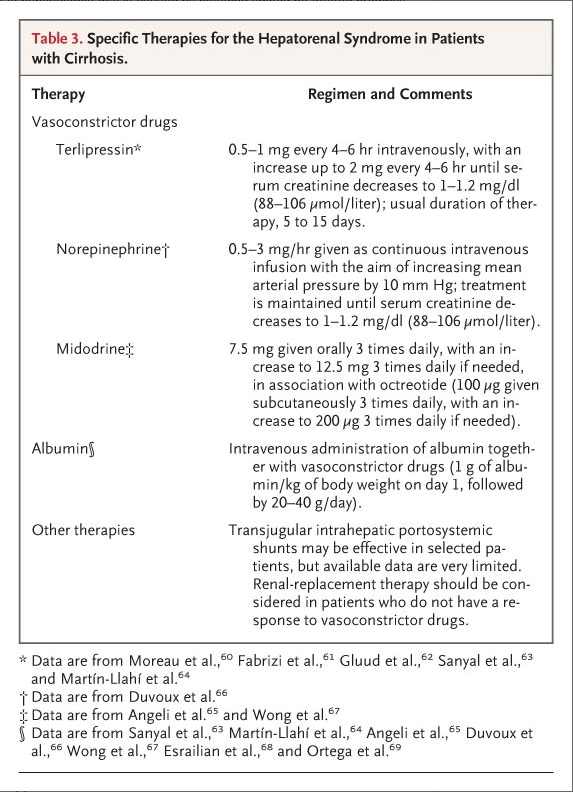
Hepatorenal Syndrome
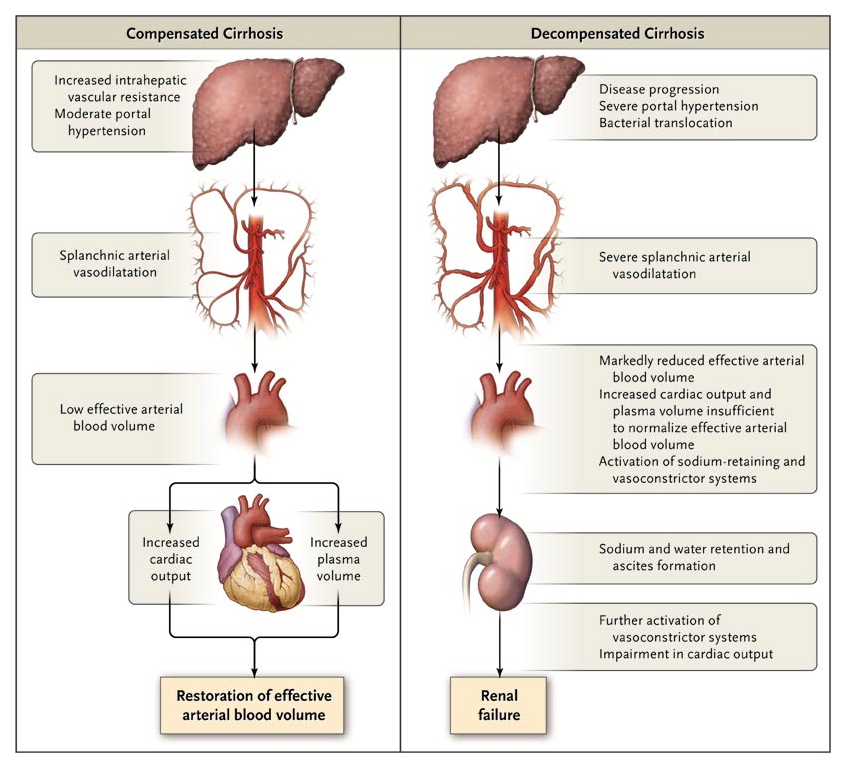
Type 1 HRS is characterized by rapid and progressive renal impairment and is most commonly precipitated by spontaneous bacterial peritonitis (SBP). Type 1 HRS occurs in approximately 25% of patients with SBP, despite rapid resolution of the infection with antibiotics. Without treatment, the median survival of patients with type 1 HRS is < 2 weeks, and virtually all patients die within 10 weeks after the onset of renal failure.
Type 2 HRS is characterized by a moderate and stable reduction in the GFR and commonly occurs in patients with relatively preserved hepatic function. These patients are often diuretic resistant with a median survival of 3-6 months. Although this is markedly longer than type 1 HRS, it is still shorter compared to patients with cirrhosis and ascites who do not have renal failure.
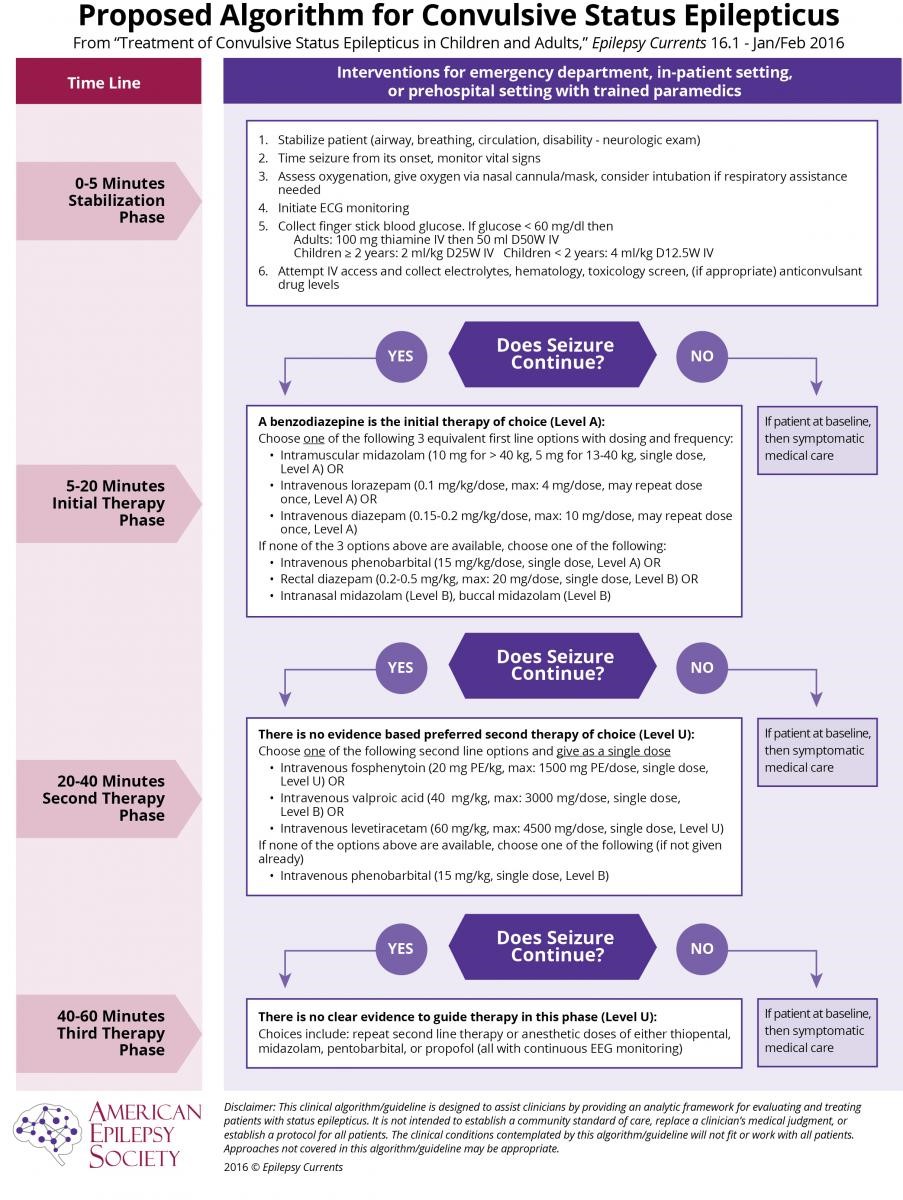
Status Epilepticus
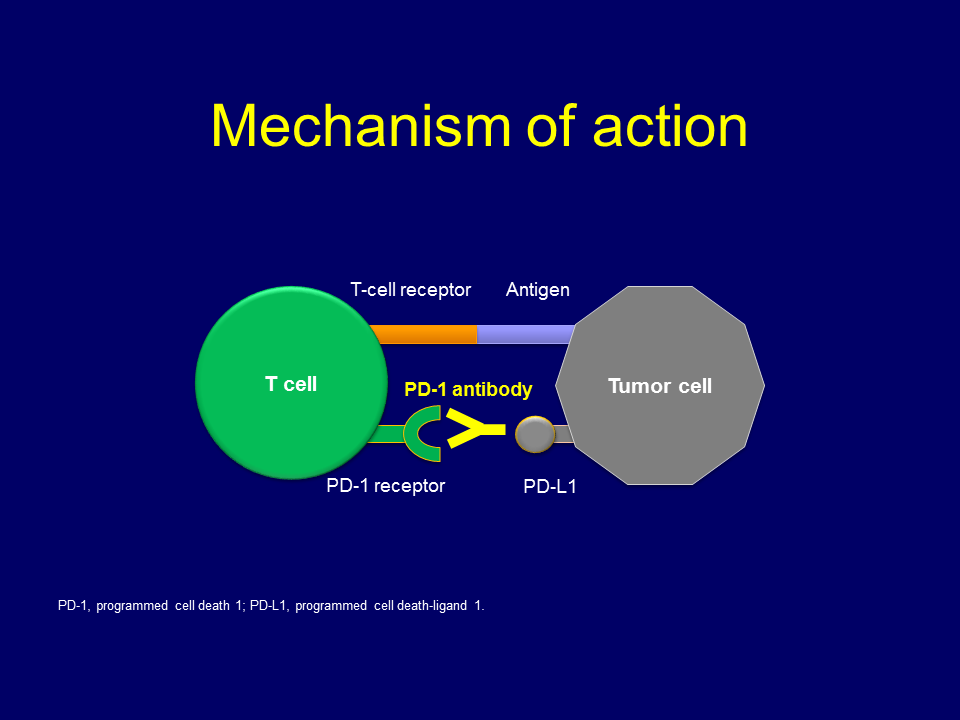
Lung Cancer Immunology Therapy: Anti-PD-1 / PD-1 Antibodies
2017 Systemic Approaches to Advance Cancer:
1. Chemotherapy
2. Molecular targets approach (Ex: EGFR Tyrosine Kinase Inhibitors)
3. Immune Checkpoint Strategies (Ex: Anti PD-1/PD-L 1 Ab)